What makes HOPE for multimorbid patients unique is its ability to manage the interplay between diagnoses – not just each diagnosis in isolation. The service is built on a rule-based AI agent that combines clinical algorithms for chronic kidney disease (CKD), hypertension, diabetes, and atrial fibrillation in a shared decision matrix. When multiple conditions are flagged simultaneously – for example chronic kidney disease and hypertension – so-called trump rules are activated that automatically prioritize the highest risk level and suggest the appropriate action. In practice, this means the system does not simply alert for a single abnormal value, but weighs the patient’s overall risk profile and accounts for the fact that an action that is right for one diagnosis may be wrong for another.
The patient registers symptoms and measurements from home via the HOPE app, connected to 4G-enabled medical devices for blood pressure, oxygen saturation, weight, temperature, blood glucose, and spirometry. All data flows in in real time and is evaluated against the individualized self-care plan. If blood pressure is too high in combination with declining kidney function, the risk level is automatically adjusted, and both patient and care team are notified of the next step. In this way, the gap between two visits is bridged – the period where deterioration otherwise goes undetected.
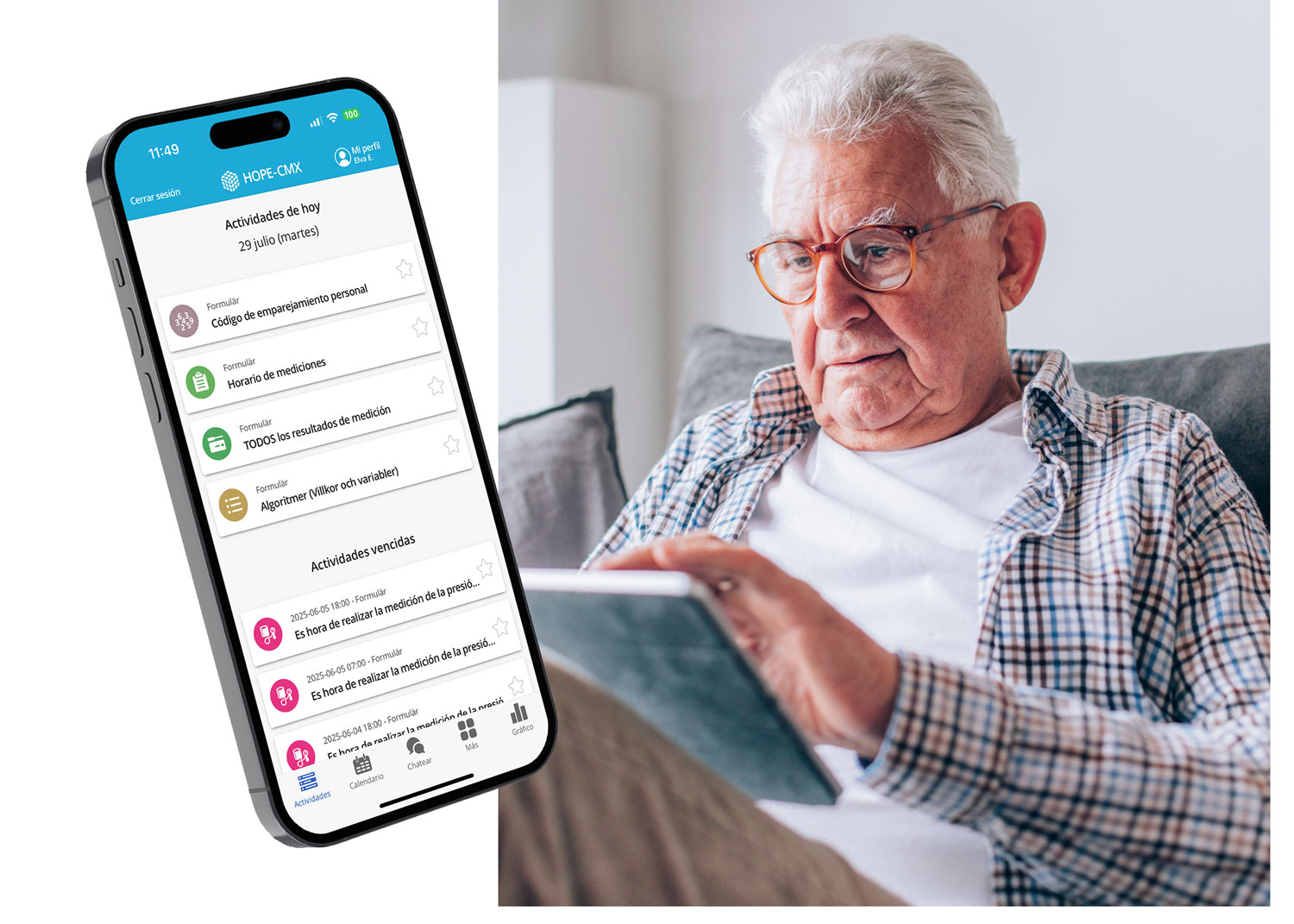
The patient as partner – not as passive recipient. Based on their registered values and symptoms, the patient automatically receives an individually tailored self-care plan – generated by HOPE without manual work from the clinic. The plan clearly shows what is normal, when the patient should act on their own, and when it is time to contact healthcare. Color-coded feedback in the app – green, yellow, red – makes it easy to understand where you stand, even for those living with multiple diagnoses simultaneously. Reminders, educational materials, and direct communication with the care team create a secure structure that makes the patient a true partner in their own care – not just someone who receives instructions at the next visit.
The difference from traditional care is fundamental. Instead of waiting for the next annual visit and hoping nothing deteriorates in the meantime, the patient receives daily feedback on their values and clear guidance on what they can do themselves. When the patient understands their situation, knows when to act, and feels confident doing so – then self-care becomes not just a concept but a way of working. It reduces anxiety, strengthens adherence, and prevents acute deterioration.